
These days we use a wide variety of lasers and IPLs to treat various targets in the skin. Two major targets are hair and blood vessels. But how much of the laser/IPL light is actually absorbed by these targets?
Using data from two very clever scientists (Steve Jacques and Scott Prahl) it is relatively easy to calculate the absorption of a wide range of wavelengths in both melanin and oxyhaemoglobin.
Figure 1 shows the absorption curves for both of these chromophores across the visible part of the spectrum, up to 650nm. The red and blue curves show the absorptions for oxy- and deoxyhaemoglobin, respectively. Both chromophores absorb very strongly in the blue end of the spectrum (between 375 and 450nm) and then peak again between about 530 and 590nm. You might think that the blue end would be a better choice for skin treatments, but you’d be wrong! The problem with blue light is that it doesn’t penetrate deep into the dermis very well!! So, we usually choose the 530 to 590nm range instead, which has much deeper penetration. These wavelngths can be generated by dye and KTP lasers and IPL units.
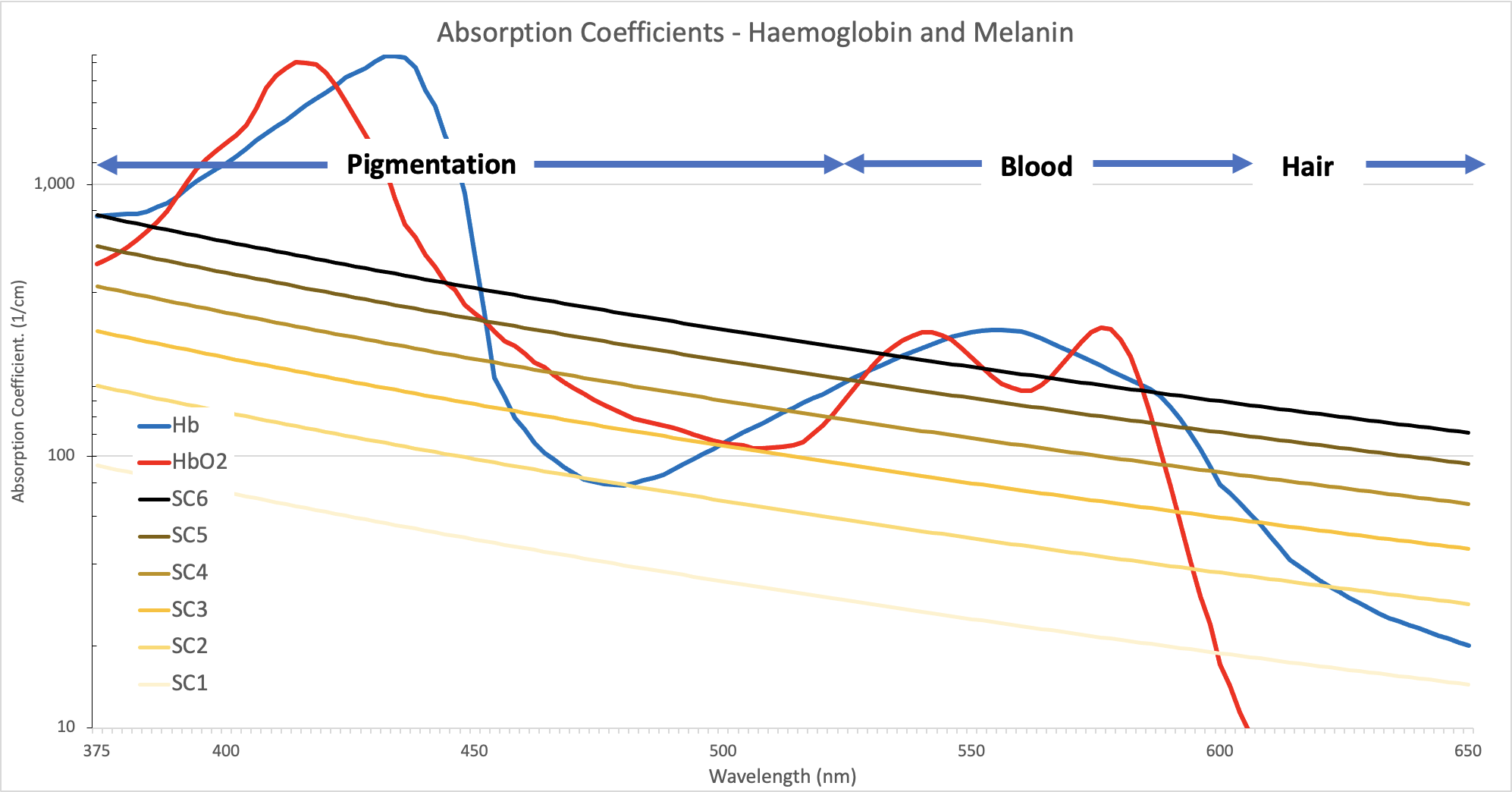
In the above diagram, the y-axis is a base 10 log scale – that means it jumps up by factors of 10s and 100s. This is done to display the curves at the lower end of the scale on the same picture as the very strongly absorbing portions. But, humans are not good at interpreting logarithmic scales, so I have created another picture to show the relations between these absorptions, more simply (I hope!).
The ‘SC1’ to ‘SC6’ curves in figure 1 represent the six major concentrations of melanin in the skin. SC1 epidermis has a melanin concentration of only 5% – very pale (commonly known as ‘Fitzpatrick 1’ – although, the Fitzpatrick scale is NOT a skin colour scale!!!). SC2 is 10%, SC3 is 16%, SC4 is 23.5%, SC5 is 33% and SC6 is 43%. These concentrations represent the change in skin colour due to melanin alone.
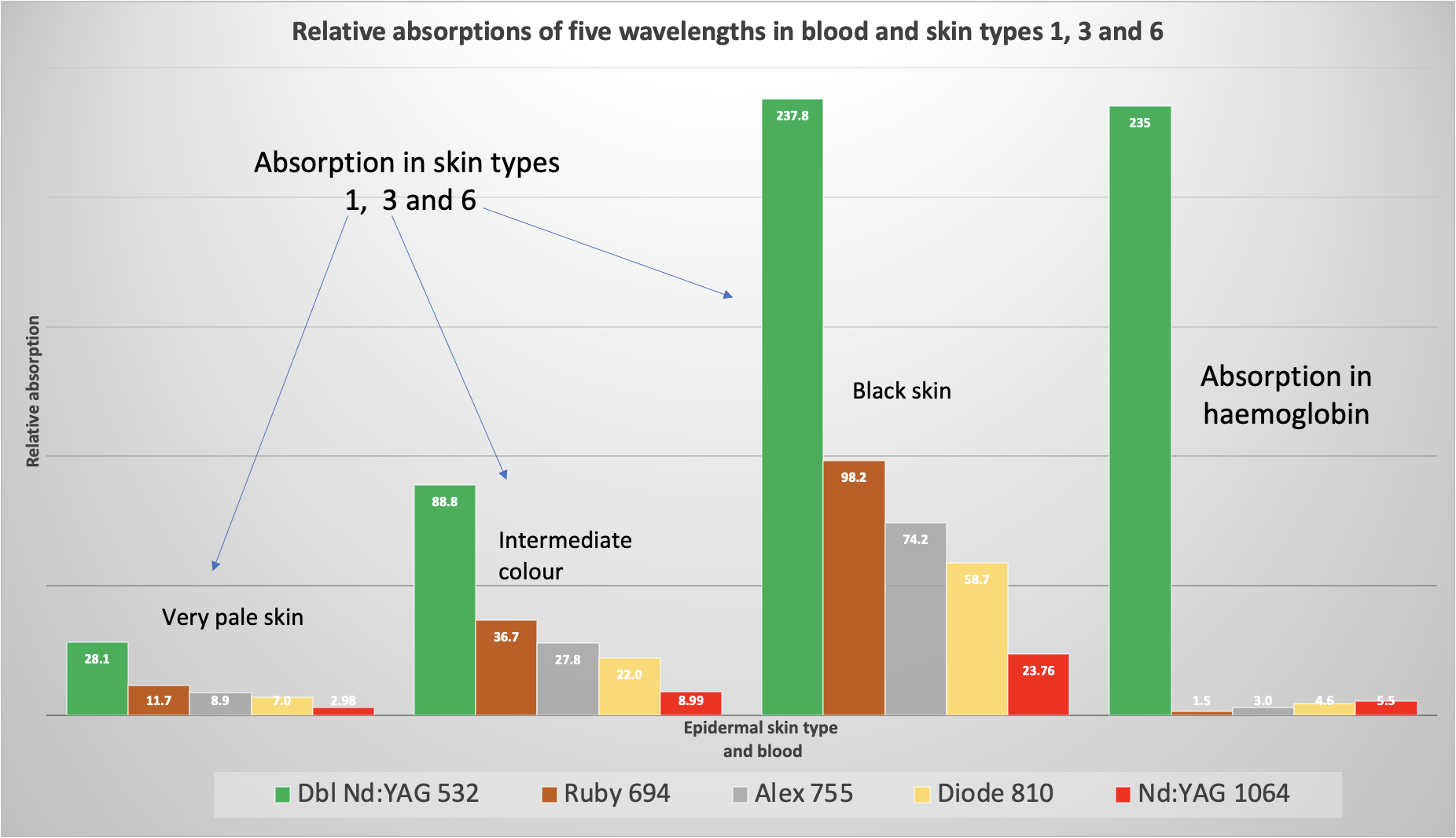
Figure 2 shows the relative absorptions of five wavelengths commonly used in laser skin treatments today, in three skin colours and haemoglobin. The skin colours I chose are SC1, 3 and 6 – which ranges from very pale skin (5% melanin concentration) to black skin (43% concentration). Obviously, the darker skin colour absorbs much more light energy than the lighter colours. This is not surprising since the higher concentration of melanosomes will obviously absorb more light. We can also see that the 532nm wavelength is the most strongly absorbed wavelength in all skin colours – again, this is not surprising since 532nm is more strongly absorbed than all the other, longer wavelgnths (see figure 1). While, the order of absorption is ruby, alex, diode followed by 1064 Nd:YAG, in all cases. Again, given the curves in figure 1, this is not surprising.
The last set of bars on the right of figure 2 shows the relative absorptions in blood. Once again, the 532nm wavelength dominates over all the others, in terms of absorption. Interestingly, the order of the other wavelengths is the reverse of that in melanin – Nd:YAG, diode, alex and then ruby. But these are all miniscule compared with the 532nm light!
All the bars in figure 2 are on the same scale. So, that means that they can all be compared against each other. This shows that the absorption of 532nm is almost the same in black skin epidermal melanin and in blood. This means that if you fire 532nm light energy at black skin you will likely damage both the epidermis and the superficial capillaries. In fact, this occurs in all skin colours too! I have observed this phenomenon in Caucasian skin (my own!) using a Q-switched Nd:YAG laser at 532nm – read my report here.
Conclusion
The above data seems to suggest that the 532nm wavelength is the ‘best’ choice for both melanin and blood vessels. However, this wavelength is strongly scattered in the dermis which significantly reduces its penetration. This makes it pretty useless when tackling hair follicles – they are too deep! Nor is it useful for deeper blood vessels. This is why the longer wavelengths tend to be used for these targets. However, 532nm is an excellent choice for epidermial pigmented lesions such as freckles, age and liver spots.
The above describes how well different wavelengths are absorbed in two main targets in the skin, but it does not describe the whole situation. For example, I have not menionted scattering much here – that’s for another day (You might want to read my report on this topic here). Nor have I mentioned ‘useful’ fluence – the fluence that actually does the task in hand. I’ll cover that topic another time.
I hope this helps you to better understand how the light we fire at skin, from our lasers, interacts with those targets.
Mike.
